50 year old male came to casualty with c/o fever since 10 days
This is an online e log book to discuss our patient identified health data shared after taking his/her guardian signed informed consent. Here we discuss our individual patient problems through a series of inputs from available global online community of experts with a aim to solve those patients clinical problem with collective current best evidence based inputs.This blog also reflects my patient centered online learning portfolio and valuable inputs on the comments box is welcome.I have been given this case to solve in an attempts to understand the topic of patient clinical data analysis, to develop my competency in reading and comprehending clinical data including history, clinical finding, investigation.
A 50 year old male came to casualty with c/o fever since 10 days
HOPI - patient was apparently asymptomatic 10 days back, then he developed fever, insidious in onset, associated with chills and rigors , and it was relieved on medication
H/o cough with sputum, whitish in colour, non blood stained.
H/o SOB ( grade 1-2 )
No H/o orthopnea, PND, chest pain.
No H/o burning micturition , decreased urine output, pedal oedema.
No H/o bleeding manifestations.
PAST HISTORY- Not a k/c/o HTN, DM, CVA, CAD, TB, Asthma, or thyroid disorders.
PERSONAL HISTORY-
Diet - mixed
App- normal
Sleep- adequate
B and B - regular
Addictions- pan daily
Allergic history:-
No history of any kind of allergies to food/drugs
Family history:-
No significant family history





GENERAL EXAMINATION:-
THE PATIENT IS CONSCIOUS COHERENT AND COOPERATIVE , WELL ORIENTED TO TIME, PLACE AND PERSON.
NO PALLOR ; ICTERUS; CLUBBING; CYANOSIS; ODEMA ; LYMPHADENOPATHY
TEMPERATURE:- 98.2F
PR:92bpm
BP:90/60 mmHg
RR:17cpm
SYSTEMATIC EXAMINATIONS:-
CVS:S1 S2+,NO MURMURS
CNS: NAD
RS:BAE+ ; NVBS
P/A:SOFT ; NON TENDER ; NO ORGANOMEGALY
PROVISIONAL DIAGNOSIS:- fever under evaluation.
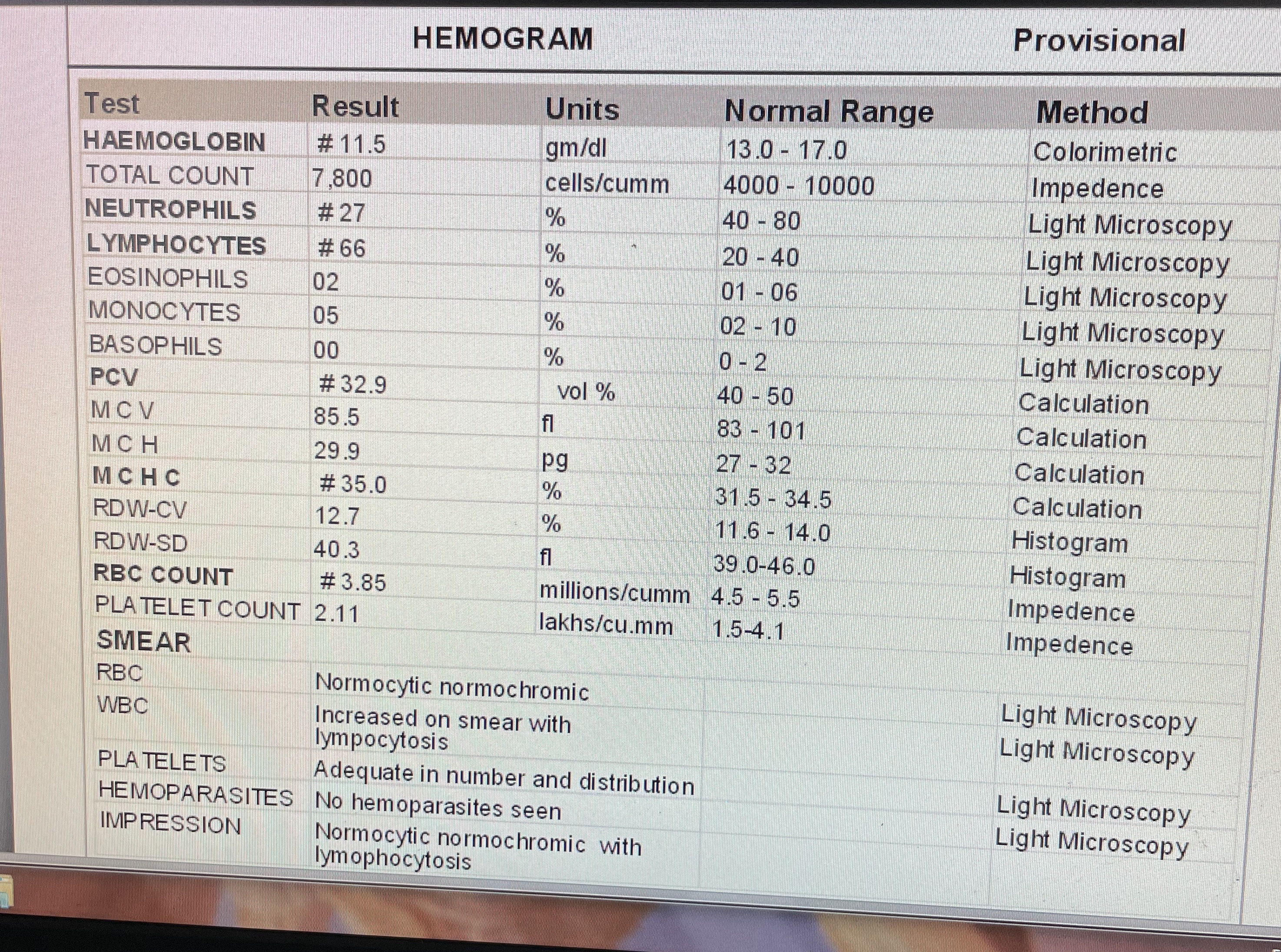
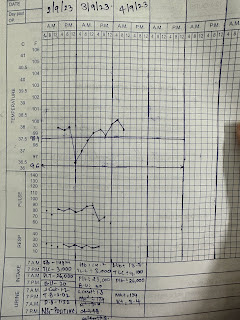
Investigations-






Comments
Post a Comment