A 70year old female came to opd with lower backpain
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome. I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
A 70 year old female came to opd with lower back pain and fever
CHIEF COMPLAINTS:-
Lower back pain since 4 days
Low grade fever since 10 days
HISTORY OF PRESENTING ILLNESS:-
Patient was apparently asymptomatic 4 years back, then she came to causality with pain in right hip and was unable to walk and was diagnosed with right femur fracture, due to fall from an auto then she was operated in our hospital ( proximal femoral nail ).
3 1/2 years ago she developed post menopausal bleeding and white discharge per vagina, so came to OBG department for checkup and was diagnosed with carcinoma of cervix II B and she underwent radiotherapy at MNJ for 5 weeks in 2019.
14 days back, she presented with abdominal pain in the left hypochondriac region, the pain was relieved on vomiting. The vomit is usually the food she consumed which is not foul smelling or blood stained and non bilious. She was diagnosed with Acid peptic disease (APD).
On investigations she had was diagnosed with anemia (low haemoglobin - 4.6 mg/dl ) for which she had 2 packs of blood transfusion and she was discharged 8 days back.
On investigations she was diagnosed as pernicious anemia.
4 days back, she came to opd with lower back pain, associated with fever since 10 days and is not associated with vomiting. The pain is continuous, dull aching and not radiating. Not associated with tenderness. There are no aggravating factors and pain was temporarily relieved on medication.
Fever is associated with generalised weakness.
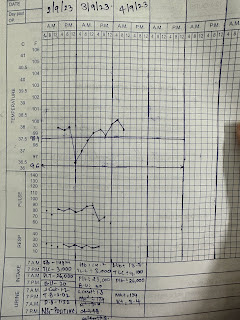
FEVER CHART:-

PAST HISTORY:-
20 years ago she was diagnosed with hypertension.
4 years back she had proximal femur nail operation for femur fracture.
No history diabetes mellitus, epilepsy, TB, asthma, thyroid abnormalities.
PERSONAL HISTORY:- ( daily routine )
She lives with her daughter, she has only one female child.
She works in a school as aaya from past 23 years.
She usually wakes up at 6 AM in the morning, but from past few days she wakes up at 8 AM .
Usually after waking up at does all the household work.
She consumes breakfast like idli, dosa, Upma, etc. at around 7AM and goes to school by 8AM.
She usually packs lunch for herself from home and consumes at 2 PM.
She comes back from school by 6 PM and cooks dinner, consumes rice with curry and takes bath and sleep by 9PM to 10PM.
She consumes diet rich in carbohydrates like rice , etc and consumes both veg and non veg .
She consumes tea 3 times per day from past 50 years.
Currently her appetite has decreased which leads to irregular bowel and bladder movements. She didn’t defecate from past 3 days.
She has no addictions.
No allergies.
TREATMENT HISTORY:-
Tab. Atenolol for hypertension.
Chemo radiation 4 years ago for 5 weeks.
She had blood transfusion 15 days back .
RADIATION THERAPY:-

FAMILY HISTORY:-
No similar complaints in the family.
GENERAL EXAMINATION:-
Patient is conscious, coherent, uncooperative and well oriented to time, place and person
Moderately built and moderately nourishment.
Vitals :-
Temp - afebrile
BP - 130/90 mm/hg
Pulse rate - 86 bpm
Respiratory rate - 13 cycles per minute
Pallor - present
Icterus - absent
Cyanosis - absent
Clubbing - absent
Lymphadenopathy - absent
Oedema - absent





Tongue- papilla absent and is smooth
Hyperpigmented lesions on tongue.
SYSTEMATIC EXAMINATION:-
1) CVS examination:-
- S1 S2 heard
- murmur heard in aortic area.
2) abdominal examination:-
Abdomen is soft and non tender
No organomegaly
No shifting dullness
No fluid thrill
Bowel sounds heard
3) Respiratory examination :-
- Chest bilaterally symmetrical, all quadrants
moves equally with respiration.
- Trachea central, chest expansion normal.
- Resonant.
- Bilateral equal air entry, no added sounds heard.
4) CNS examination :-
- No focal neurological defects.
- all cranial neves are intact.
GCS:- 15/15
Power:-
Rt UL-5/5. Lt UL-5/5
Rt LL-5/5. Lt LL-5/5
Tone:-
Rt UL -N
Lt UL-N
Rt LL-N
Lt LL-N
Reflexes: Right Left.
Biceps. ++. ++
Triceps. ++ ++
Supinator. ++ ++
Knee. ++ ++
Ankle. ++ ++
Plantar: Flexion Flexion
PROVISIONAL DIAGNOSIS:-
Fever under evaluation with lumbar spondylosis.
Pernicious anemia.
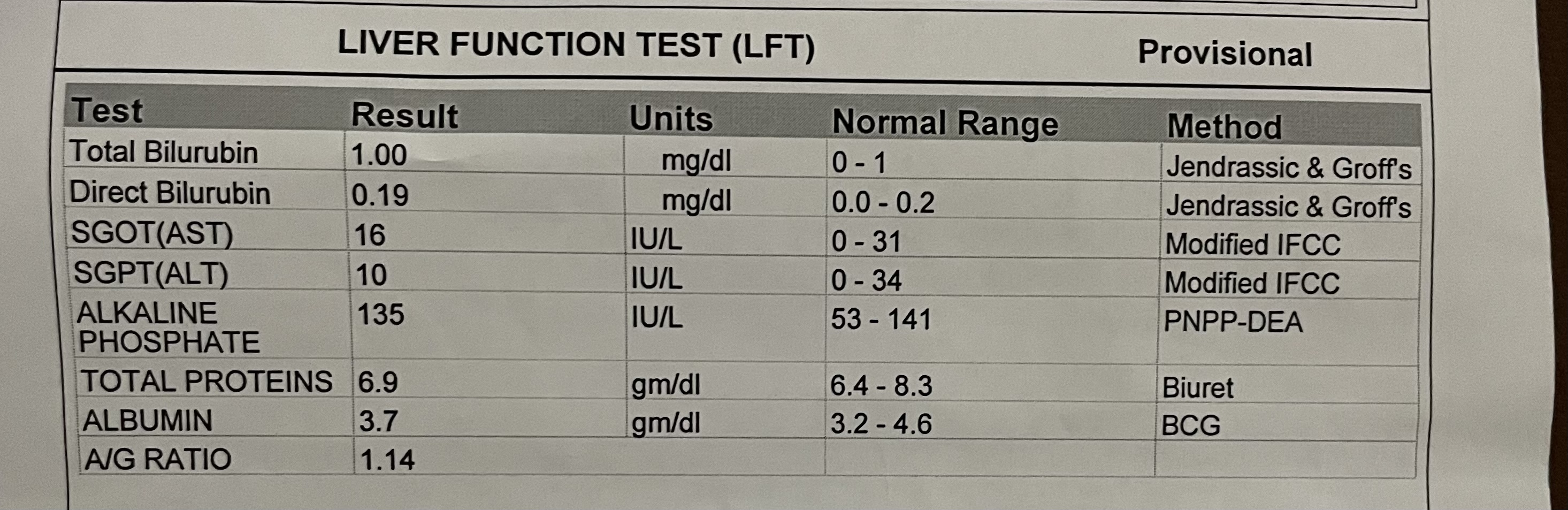
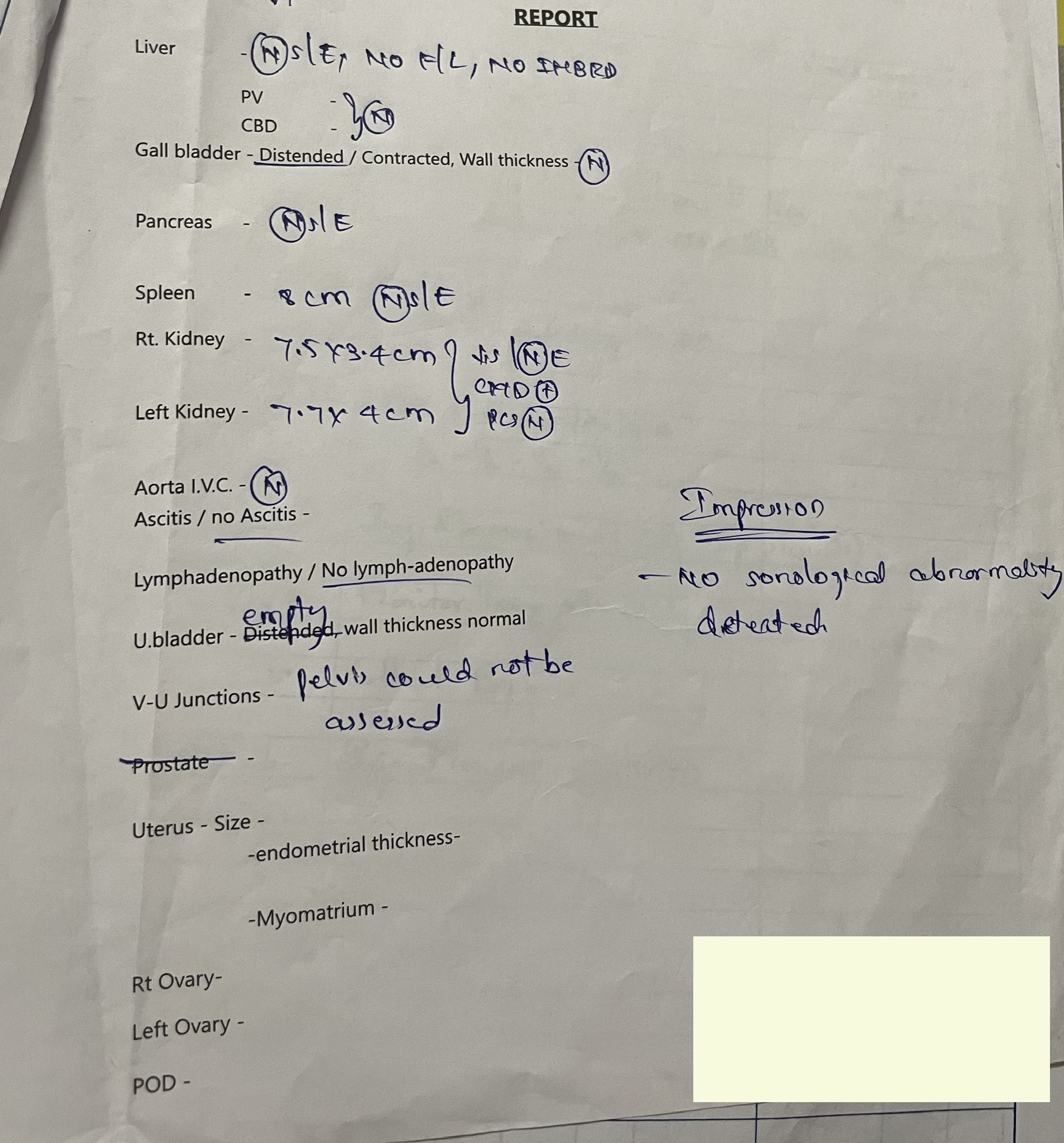
INVESTIGATIONS:-
X-RAY:-
Lateral view:-














TREATMENT:-
Tab Dolo 650mg / PO / TID
Inj Neomol 100ml/ IV/ SOS
Tab Ultracet 1/2 PO/ QID
Tab Livogen / PO / OD
Tab Shelcal - CT/ OD - 15 days
Volini gel for L/A
A to Z syrup PO/ TID
Monitor vitals
T Amlong 5mg / PO /TID


Comments
Post a Comment